
- Helpline No.
+91-9001867424
- 123/1, Mahaveer marg
Mansarovar, Jaipur

Benign Prostatic Hypertrophy (BPH)
The prostate is a small, chestnut-shaped gland in the male reproductive system. Only men have a prostate. It is composed of different lobes enclosed in a fibrous capsule. Located in front of the rectum and just below the urinary bladder, the prostate also surrounds part of the urethra (the canal through which urine is carried from the bladder and out of the body through the penis) as shown in the diagram below. Diagram Showing the Location of the Prostate
The prostate contributes to the milky fluid that carries the sperm produced by the testes. The prostatic fluid is also thought to supply nourishment for the sperm. Since the prostate contributes to ejaculate throughout the better part of a man's life, many men are able to father children well into their 70s and 80s.
BPH is a non-cancerous enlargement of the prostate gland in men. BPH is commonly found in older men. Throughout childhood, the prostate is very small. It begins to enlarge during puberty and approximately doubles in size; then the growth slows down. At around the age of 45, the prostate often starts growing again and continues to enlarge for the rest of a man's life. This is considered to be due to hormonal changes.
The enlargement itself is not the problem. However, as it continues to enlarge, it can frequently start to squeeze the urethra (this is similar to what happens when a straw is pinched). This can interfere with the normal flow of urine and cause uncomfortable symptoms. An enlarged prostate generally does not interfere with sexual functioning. However, severe urinary symptoms can be embarrassing and can inhibit a man's sexual activity. Not all males suffer from the symptoms of an enlarged prostate. 4 out of every 10 men over the age of 55, 7 out of 10 men in their 70s and an even larger number by the age of 80, suffer from the symptoms of an enlarged prostate.
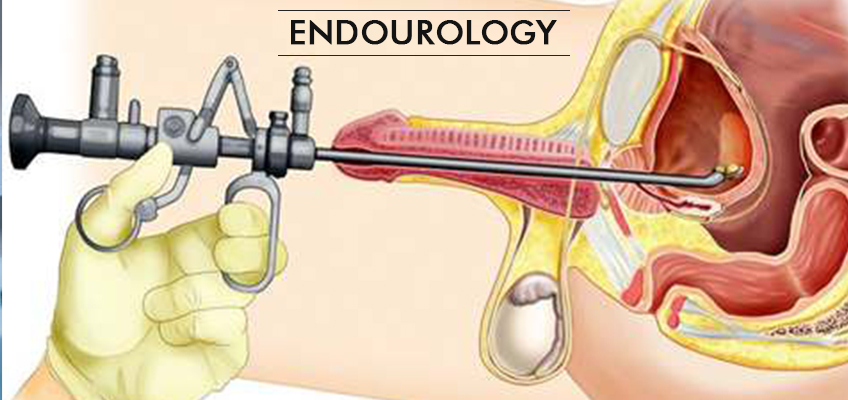
The field of endourology deals with accessing and treating urinary tract disorders using endoscopic equipment.
- TURP ( Transurethral resection of prostate) - for BPH
- PCNL (per cutaneous nephrolithotomy) - for Kidney stones
- TURBT(Trans urethral resection of bladder tumour) - for Bladder cancer
- OIU (optical internal urethrotomy) - For urethral stricture
- Difficulty in starting urination
Diagnosis & Tests for Benign Prostatic Hypertrophy (BPH)
The urinary symptoms of an enlarged prostate are one or more of the following:
- Frequent urination, especially at night
- A sudden, uncontrollable urge to urinate
- A poor urine stream
- A sense of the bladder not emptying completely
- Difficulty in starting urination
- Urinary incontinence
- Total blockage of urine
- Bleeding in the urine
- Urinary infection
BPH is usually diagnosed in the following manner or by a combination of some of the methods listed below:
- Medical History: Your doctor will take a detailed medical history, which will include past and present medical problems.
- Digital Rectal Examination: Examination of the prostate gland by inserting a gloved, lubricated finger into the rectum.
- Checking for Other Medical Problems: that may be causing similar symptoms.
- Checking of Your Urine: for the presence of infection.
- Performing a Urine Flow Test: for the measurement of urine flow. A flowmeter is used to measure the force of your urine stream and the degree of blockage.
- Performing an Ultrasound Scan: to obtain details about the prostate gland, its effects on the kidneys, if any, and the amount of urine in the bladder after urinating.
- Performing a Urodynamic Study: if needed, to check bladder pressure.
- Measurement of the Post-Voiding Residual Urine: (urine remaining in the bladder after urination or voiding) by catheterisation or ultrasound.
- Ultrasound of the Urinary Tract
- Intravenous Pyelography (A Specialised X-Ray)
- Cystoscopy (Examination of the Urinary Tract with a Special Viewing Tube)
- Conducting Other Tests: x-rays, biopsy, etc., if indicated.
Treatment for Benign Prostatic Hypertrophy (BPH)
Depending upon the severity of your symptoms, several treatment options are available. Your urologist will discuss these options with you before deciding on any one method:
About 50% of patients experience failure to ejaculate after intercourse, as the semen is pushed backwards into the bladder,instead of to the outside.
Very rarely, some people experience leakage of urine either upon straining or continuously
About 2% of patients may experience transcend or permanent impotence.
All tissue removed at the time of surgery will be sent for examination to confirm the benign nature of the gland. Very occasionally, a surprise report of the presence of malignancy may be obtained.
Treatment for BPH does not eliminate future incidence of prostate cancer, as this originates in an entirely different portion of the gland. Therefore, an annual evaluation may still be considered important for men who have undergone surgery for benign prostate gland enlargement.
Just because the prostate is enlarged, it does not need to be treated. If your symptoms are mild, you may not need any treatment at all. If your symptoms are severe, or if the result of the tests shows that the urinary tract is significantly affected, you must under-go early therapy.
Percutaneous Nephrolithotomy (PCNL)
PCNL is a procedure for removing stones in the kidney or the upper ureter Illustration Showing How PCNL is Performed
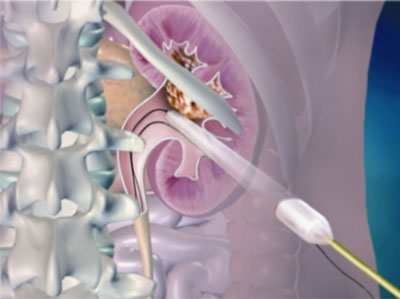
PCNL is a well-established procedure by which stones in the kidney or the upper ureter are removed by making a small incision in the flank. Generally, an incision, that is 1 cm or less than 1 cm, is made in the flank. A guide wire is passed through this incision into the kidney. This is performed under fluoroscopy or x-ray control.
A passage is then created around this guide wire by dilatation. Through this passage, a nephroscope is passed into the kidney to visualise the stone and remove it. Larger stones can be fragmented by different methods and removed. Stones are therefore cleared easily. Once the procedure is complete, a tube is left through this tract as drainage for one or two days.
The main advantage of this approach is that, unlike traditional open surgery, only a 1 cm incision is made in the flank. The stones can be visualised directly and removed. Unlike ESWL or ureteroscopy, the stones are removed in the same sitting and the kidney is cleared of calculi. The stay in the hospital is only for 3-4 days.
This surgery would be recommended as a treatment of choice, if the patient has kidney stones larger than 2 cm, upper ureteric stones bigger than 1 cm, or at times for stones found in the lower pole of the kidney that cannot be effectively treated with either ureteroscopy or ESWL. This procedure is also performed following failure of other modalities of treatment such as medical therapy, ESWL, etc., for renal and upper ureteric stones.
This procedure is commonly performed under general anaesthesia, and therefore you also need to be admitted to the hospital for this procedure. In special circumstances, it can be performed under intravenous sedation, regional anaesthesia or local anaesthesia.
The success rate of clearance of stones with this procedure ranges between 90 to 95%. This actually depends upon the size, number and location of these stones. Sometimes, complete clearance may require a second procedure after a few days.
For the post-operative course, the patient will generally need to stay in the hospital for 2 to 3 days after the procedure. He or she will also undergo additional x-rays or ultrasound studies, to determine if there are any residual stone fragments present. A large amount of residue will require the urologist to look again with a nephroscope to remove it. The other alternative is to treat the remaining fragments with ESWL. From the site of the puncture, the patient will have a drainage tube and a urethral catheter, for a day or two. Following the removal of the flank drainage tube, urine may leak for a day. Post-operatively, the urologist will also encourage a high fluid intake to keep the daily volume of urine produced to more than 2 litres a day.
By and large, this procedure is safe. Some risks that can be associated with all surgical procedures are the possibilities of bleeding (1%) and infection, sometimes requiring blood transfusion.
Some patients have prolonged leakage of urine from the flank site, requiring ureteric stenting. Fever, if present, will require a change in antibiotic.
Rare complications include persistent uncontrolled bleeding due to arteriovenous malformations or pseudo-aneurysms (0.4%), which would need secondary procedures or even a nephrectomy to control the same. When a supracostal puncture (above the 12th rib) is made, complications would then include pneumothorax (commonly called collapsed lung caused due to the accumulation of air or gas in the space surrounding the lungs) or fluid accumulation in the thorax. Again, the incidence of these is only 0-4%.
The time by which a patient can get back to work would depend upon the magnitude of the stone burden and the number of tracts made. Most patients return to average activity levels within a week or so. A return to vigorous activity should probably take place after two weeks.
The contraindications to this procedure are bleeding disorders and pregnancy (due to the risk of radiation). The others are medical problems making the patient unsuitable for anaesthesia.
It is advisable to maintain a urine output of 2 to 2.5 litres per day. Your doctor may also advise dietary changes and medications, which will be individualised. Generally a high-fibre diet, with avoidance of high-calorie foods, is recommended.
Separate and specific changes in the diet may be suggested in case of other conditions associated with urinary stones.
Flexible Cystonephroscope
At Ideal urology hospital we utilise the ACN 2-ACMI flexible cystonephroscope. This permits painless cystoscopy (visualisation of the urinary bladder), ureteric stent removals and the stenting of ureters. It is also utilised during PCNL for achieving complete stone clearance by retrieving other smaller calyceal or ureteric calculi. The ACN 2-ACMI flexible cystonephroscope has a 14.6 Fr diameter with a working channel of 6.4 Fr and an active deflection of 180 degrees up and 170 degrees down.
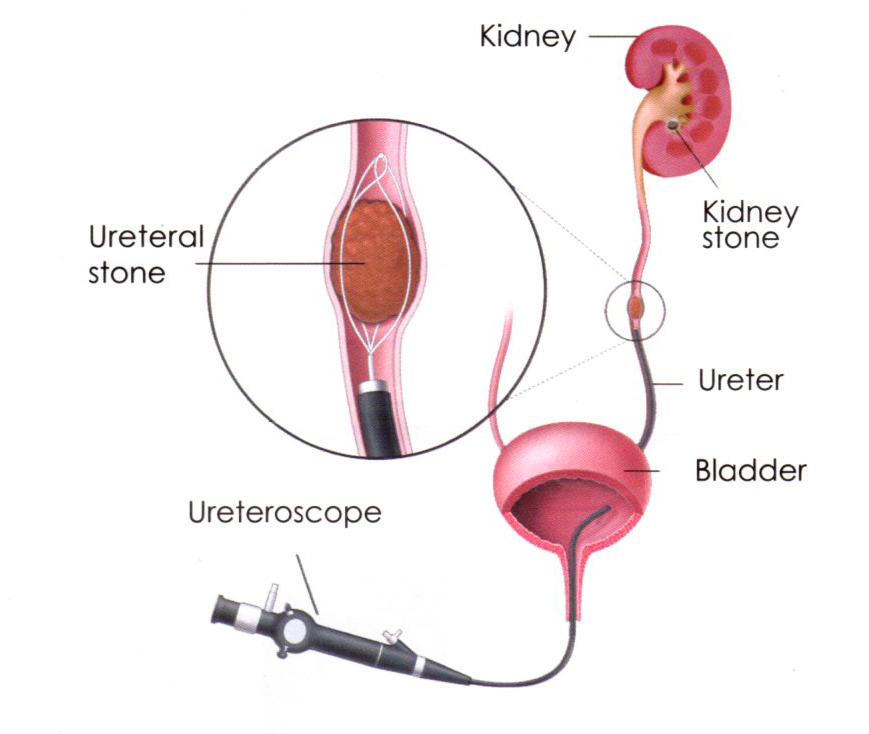
Flexible Ureteroscope
Flexible ureteroscope is utilised for both diagnostic and therapeutic retrograde intrarenal surgery (RIRS). It can be used for lithotripsy and stone extraction in the ureter or the kidneys. It enables access to the entire renal tract including the lower renal calyx. It also enables detection of pathologies in regions where access is difficult.
The flexible ureteroscope can be used in diagnostics for:
- Identifying the causes of haematuria
- The differential diagnosis of filling defects
- The observation of ureteral tumours
It can be used in therapy for the:
- Removal of calculi / foreign bodies
- Treatment of ureteral tumours
- Coagulation of haemorrhages
- Disintegration of ureteral stones
- Removal of necrosed papillae
Paediatric Endoscopes
The entire gamut of paediatric endoscopes for both the upper and lower tracts is available. These include cystoscopy, resectoscope, urethrotome, ureteroscope and nephroscope. We are one of the few centres that are equipped to operate on the entire range of paediatric urology disorders. For more details, please click here to go to the section on paediatric urology.


